
Tools: Stopping or Not Starting Treatment in Dementia Care
Defining Severe Enough

When I was a Hospice Nurse Practitioner on an inpatient unit, I bumped up against existential suffering a lot. Unfinished business, ruined relationships, soul deep regrets of all kinds. Needless to say I learned a ton from my time with the chaplains I worked closely with and still turn to now with my own suffering.
This week I looked at a paper from Dr. Stanley Terman and others in the San Francisco Bay area who challenge us to broaden the concept of suffering in advanced dementia. Dr. Terman is a psychiatrist and bioethicist. I was fascinated.
I should back up and say the majority of my professional life was caring for cancer patients. When someone came in and said they were “done” with treatment. It was usually clear that the side effects from modestly effective treatment were not worth it anymore. They wanted the time they had left to be high quality. Really kind of a no brainer.
That is never the situation at end of life with dementia patients who have lost capacity to make decisions for themselves. Which leaves us to rely on what Terman calls precedent autonomy—decisions made previously but still within their right to self-determination.
Critics would say, the treatments advanced Alzheimer’s patients would choose to stop or not start, are generally treating something else, not focused on stopping or slowing advanced dementia, the way chemotherapy is about stopping or slowing the growth of metastatic tumors. Nevertheless bioethics are clear that patient’s can refuse medical treatment as a core component of self determination.
However, Alzheimer’s is like cancer in that it is a terminal disease and one society largely dreads, as some dread the spectre of a cancer diagnosis, but in some ways Alzheimer’s is dreaded moreso because of the slow withering away of personhood.
Terman argues that if people living with dementia have documented with forethought, when they feel their decline would constitute “severe-enough suffering” to opt out of any life prolonging care, while they still had decision making capacity, that represents precedent autonomy and aligns with the American Medical Associations Code of Ethics Opinion 2.20 that reads “The social commitment of the physician is to sustain life and to relieve suffering. Where the performance of one duty conflicts with the other, the preferences of the patient should prevail.
Terman describes how the word severe in this context does not imply intensity as in rating scales, but rather severe in this context represents “enough” suffering to want to be allowed to die. He goes on to describe five types of suffering in advanced dementia: physical, psychic or emotional, existential, disruption of life narrative, and loved one’s suffering (see the table below).
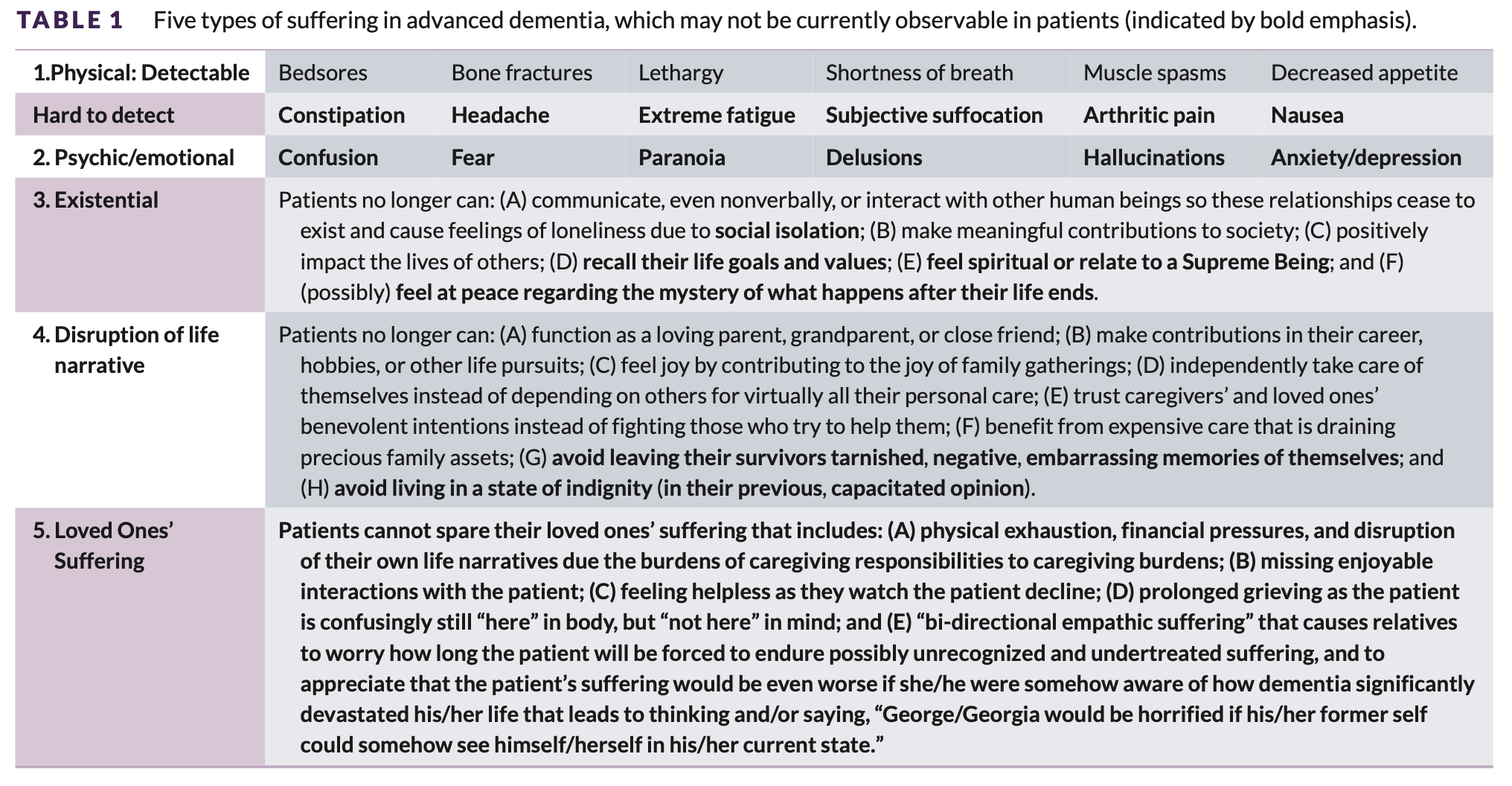
The term “bi-directional empathic suffering” that appears in bullet point #5 left me crying (again), as I remembered one poignant moment. I was on the floor cleaning up the aftermath of my soulmates incontinence. I looked up at him standing in the shower. Our eyes met and I saw in his eyes that he recognized the heartbreak in my eyes at what the disease was doing to him. A flash of horror at the suffering he was causing in his eyes before he turned away.
But I digress.
Terman goes on to argue the concept of “severe-enough suffering” should serve as criteria for a person living with dementia to be allowed to die through opting out of any life prolonging care including hand-feeding. In this article he is focused on the role of the physician as a partner in decision making but I always think about the Durable Power of Attorney for Healthcare or proxy medical decision maker.
How does a proxy know when someone is at severe-enough suffering. In cancer care we routinely used worksheets for identifying the patient’s life values and medical treatment preferences during goals of care conversations we had, often at the time of disease progression.
I use a similar worksheet to assess when someone would want to opt out of life prolonging care as an addendum to a dementia-specific health care directive in the agree/disagree format that we used to assess values and preferences. The proxy decision maker still has to make the decision in real time, but this kind of tool serves to remind and underscore for them, when their loved one might agree or strongly agree that it is time to stopping life prolonging care.
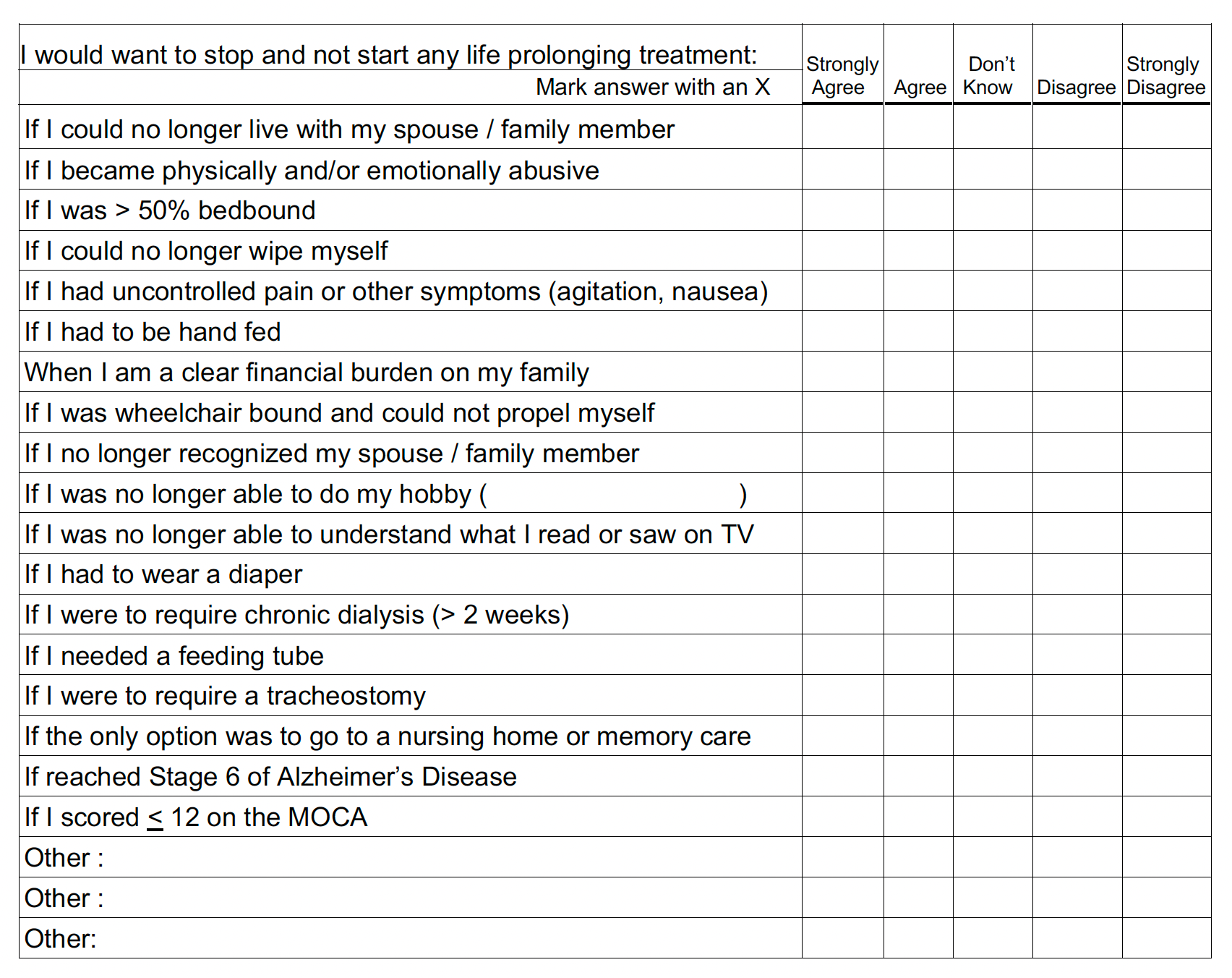
Download the pdf of the stop and don’t start tool for free at this link annadupen.com/downloadable
Consider supporting my work with a $5 monthly subscription
Learn about Dementia-Specific Health Care Directives at